- Article

Transcatheter Versus Sutureless Aortic Valve Replacement: A Propensity-Matched Single-Center Cohort Study
- Nikoleta Stanitsa,
- Emmanouel Tempelis and
- Panagiotis Dedeilias
- + 5 authors
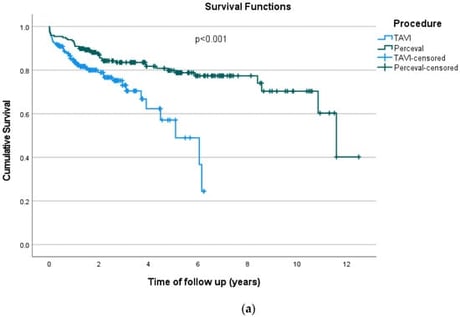
Background and Objectives: Over the past decade, transcatheter aortic valve replacement (TAVI) has evolved from a treatment for inoperable patients to an established option across all risk categories. In parallel, the Perceval sutureless valve has demonstrated safety and efficacy especially for minimally invasive surgical aortic valve replacement (AVR). Despite the advances of both TAVI and Perceval, robust long-term data and clear patient selection criteria are still lacking. This retrospective single-center study reports the outcomes of patients undergoing isolated AVR with the Perceval sutureless valve or with TAVI. Materials and Methods: We retrospectively reviewed consecutive patients undergoing isolated AVR at our institution between April 2013 and December 2024. Of 1006 eligible patients (424 TAVI; 582 Perceval), propensity score matching was performed for age, sex, EuroSCORE II, body surface area, and comorbidities, yielding 197 matched pairs. Primary endpoints were all-cause and cardiovascular mortality. Secondary endpoints included acute kidney injury, permanent pacemaker implantation, stroke, pericardial effusion, ICU stay, and overall hospital stay. Clinical and echocardiographic follow-up was obtained by medical-record review and routine echocardiography, with an additional prospective clinical and echocardiographic evaluation at 6–12 months. Results: Postprocedural paravalvular leak was significantly more frequent after TAVI than after Perceval AVR (23.4% vs. 2.5%; p < 0.001). At 6–12 months, TAVI was associated with greater aortic regurgitation and higher rates of para- and intra-prosthetic leak (both p < 0.001) and higher mean transvalvular gradients, particularly in small and medium valve sizes. ICU and overall hospital stay were longer after Perceval implantation (both p < 0.001). New permanent pacemaker implantation was numerically higher after TAVI (11.2% vs. 5.6%; p = 0.063). Early mortality was similar; however, 1-year mortality was higher after TAVI (16.2% vs. 9.1%; p = 0.045), and Kaplan–Meier analysis demonstrated better overall survival with Perceval (p < 0.001), while cardiovascular survival did not differ significantly (p = 0.851). Conclusions: Our study underscores the importance of meticulous patient selection when choosing between TAVI and Perceval. Perceval implantation was associated with better long-term overall survival than TAVI in the propensity-matched cohort. Paravalvular leaks were more frequent after TAVI and associated with poorer survival. Both approaches achieve excellent outcomes; however, differences in long-term survival and valve performance highlight the need for a personalized treatment strategy guided by a multidisciplinary heart team.
3 March 2026